
Diaphragmatic hernia
What’s that?
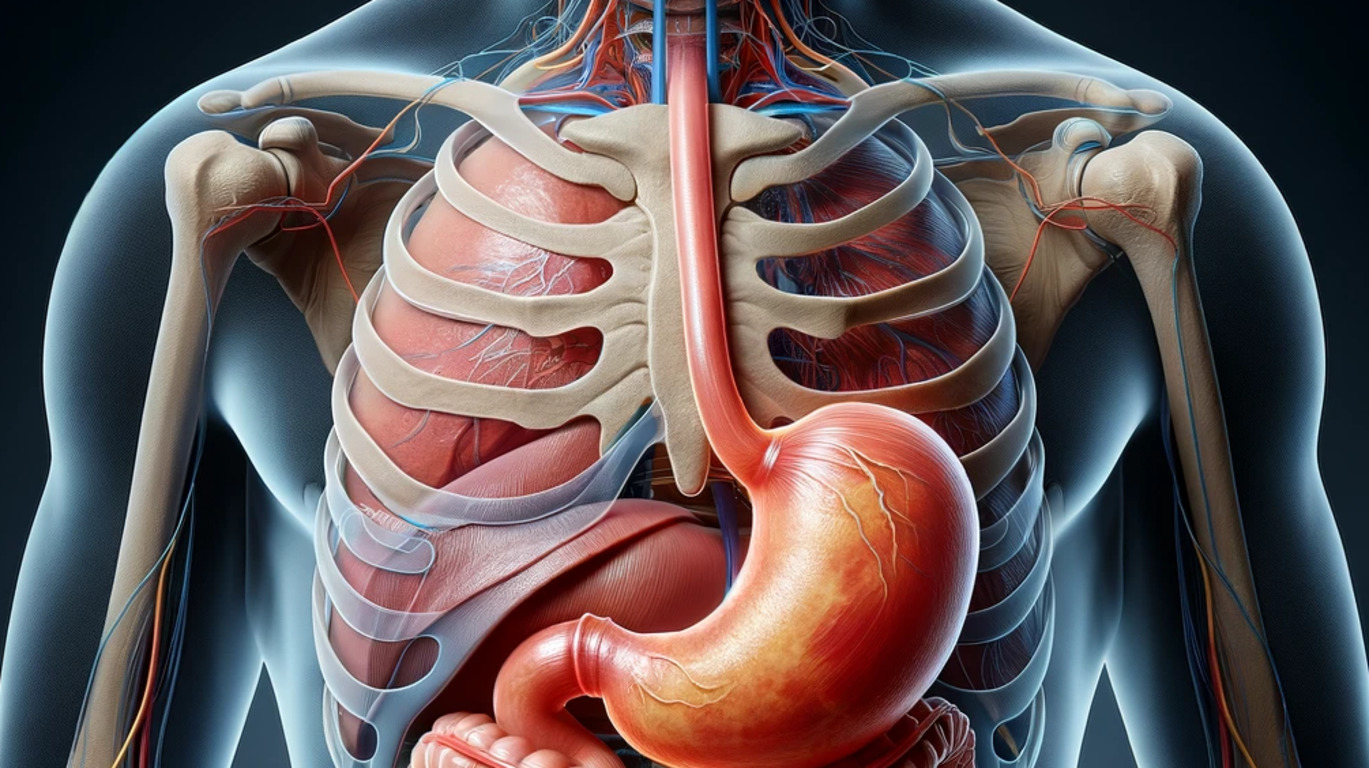
Diaphragmatic hernia is a chronic pathology, which is characterized by the protrusion of parts of the abdominal organs into the thoracic cavity through an opening in the diaphragm.
About the disease
Abdominal organ displacement can result from either artificially formed defects (such as those caused by trauma or wounds) or weaknesses, particularly in the region of the diaphragm’s esophageal opening. This can lead to the protrusion of the abdominal section of the esophagus (approximately 2 cm in length), the upper portion of the stomach, and occasionally intestinal loops. Diaphragmatic hernias may be congenital or acquired, with a 5% prevalence among adults, half of whom remain asymptomatic, often discovering the condition incidentally during examinations for unrelated issues.
Axial hernias are the most common, accounting for 98-99% of cases, characterized by the protrusion of the abdominal esophagus and the upper part of the stomach into the thoracic cavity, while the thoracic portion of the esophagus forms a single tube. These hernias are typically non-fixed, meaning the herniated contents revert to the abdominal cavity when positions are changed. Paraesophageal hernias occur at a frequency of around 1.5%, where the protruding organs are positioned alongside the normal esophagus. In less than 1% of cases, diaphragmatic hernias can be linked to a congenitally short esophagus.
Typical symptoms of diaphragmatic hernia are pain in the epigastric zone, left or right side of the chest. In addition, a person is bothered by a feeling of heaviness, shortness of breath and palpitations, with these signs appearing soon after eating. On an empty stomach, there is no symptomatology, which makes the patient consciously limit food intake. After eating, a single vomiting may occur, which contributes to relief. Similarly, bowel emptying affects the subjective sensations of the patient. The pathognomonic symptom of diaphragmatic hernia is “gurgling” or rumbling on the right or left side of the chest cavity, as well as difficulty breathing when moving to a horizontal position. The change of symptomatology depending on the position of the body is an important differential diagnostic sign.
Diagnosis of hernias is based on the results of radiological examination, which allows visualization of the herniated area. However, small axial hernias may not be visualized in the standing position, so a horizontal scan is recommended.
Treatment of diaphragmatic hernia begins with conservative measures, which are aimed at eliminating reflux gastritis and pathological symptoms. If such therapy is ineffective or if complications develop, the question of surgical intervention is decided.
Types of diaphragmatic hernia
According to the pathogenetic classification, there are 2 main types of diaphragmatic hernia:
- true – weaknesses in the diaphragm are associated with a local absence of muscle fibers, with the weaknesses represented only by connective tissue, which is the hernia sac;
- false – these are absolute defects in the diaphragm congenital or acquired, through which the abdominal organs protrude, with only a hernia hole, and no hernia sac.
According to topography, axial and paraesophageal hernias are distinguished.
There are also 3 degrees of severity of axial hernias:
- First – only the abdominal part of the esophagus penetrates into the thoracic cavity, with the stomach in close contact with the diaphragm, but remains in the abdominal cavity;
- Second – only the abdominal segment of the esophagus remains in the thoracic cavity, and the stomach is in the diaphragmatic opening;
- Third – the abdominal segment of the esophagus and part of the stomach are in the thoracic cavity.
Symptoms of diaphragmatic hernia
The primary symptom of diaphragmatic hernia is pain, which varies in intensity from dull to sharp. This pain often changes with body posture, becoming less intense when standing upright. The pain frequently radiates to various body parts. Another common symptom is heartburn, often triggered by meals and sudden changes in body position, such as bending forward or lying down. Night heartburn, linked to increased parasympathetic nervous system activity that relaxes the lower esophageal sphincter, is also typical.
Patients with diaphragmatic hernia, particularly when the hernia is on the left side, may experience “cardiac” symptoms due to the hernial contents exerting direct mechanical pressure on the heart. These symptoms include rapid, uncomfortable heartbeats and chest pain on the left side.
In cases where organs have moved into the chest cavity and become trapped (impinged hernias), symptoms become severe and acute. This includes sudden, intense pain in the lower chest or upper abdomen, and a feeling of pressure on the affected side in the thoracic cavity, which intensifies with the size of the trapped organ. Impingement disrupts blood circulation, leading to plasma leakage and lung compression, manifesting as increased difficulty in breathing. If blood flow is severely impaired, the trapped organ can undergo necrosis, potentially perforating into the chest cavity. This leads to extreme chest pain, a decrease in blood pressure, and possibly loss of consciousness. If the contents of the perforated organ leak, peritonitis can develop within hours.
Causes of diaphragmatic hernias
Causes of diaphragmatic hernias can be congenital and acquired. They are often associated with the following factors:
- excessive fatty tissue in the body;
- poor posture;
- chronic cough;
- chronic constipation;
- aggravated heredity;
- tobacco smoking;
- developmental anomalies;
- traumatic injuries.
The occurrence of diaphragmatic hernia is the result of a combination of 3 factors:
- connective tissue disorders;
- high pressure inside the abdominal cavity;
- esophageal motility disorder.
Congenital diaphragmatic hernia is the result of abnormal embryonic development of the diaphragm. There are indications of hereditary nature of this anomaly, in 10% of observations there is a connection with chromosomal abnormalities. The etiologic role of toxic effects on the fetus during pregnancy is not excluded. Congenital diaphragmatic hernia is the result of impaired embryonic development of the diaphragm.
Diagnosis of diaphragmatic hernia
Standard radiologic examination is the first diagnostic method. The diagnosis is confirmed by the detection of hollow abdominal organs in the thoracic cavity, elevation of the diaphragmatic dome on the affected side, and displacement of mediastinal organs on the opposite side.
Often the diagnosis of diaphragmatic hernia includes a CT scan. In most cases, CT scanning allows to accurately diagnose, assess the localization (anterior, posterior, lateral), size, characteristics of the hernia, and determine the patient’s management tactics.
Magnetic resonance imaging visualizes the entire diaphragm and shows a clear differentiation of its structures. The method allows you to establish the exact localization of the site of damage and measure the herniated protrusion.
In about 15-20% of patients with diaphragmatic hernia, pain sensations are localized in the heart area and are mistaken for cardiac pathology. As part of differential diagnosis, electrocardiography and ultrasound scanning of the heart are indicated.
Treatment of diaphragmatic hernia
According to clinical guidelines, conservative treatment of diaphragmatic hernia is the first line of treatment. Surgery is performed if indicated.
Conservative treatment of diaphragmatic hernia
Conservative therapy is aimed at combating reflux esophagitis, which is characterized by inflammation of the esophageal mucosa against the background of acidic gastric contents. For this purpose, medication and non-medication measures are recommended. The latter include compliance with the principles of dietary nutrition, refusal to smoke and drink alcoholic beverages, reducing excess weight, lifting the head end of the bed during sleep. After eating, it is recommended to stay in an upright position for some time.
Medication treatment consists of the following:
- use of proton pump inhibitors, which make gastric contents less aggressive (block the secretion of hydrochloric acid);
- use of antacid preparations to neutralize the acidity of gastric juice;
- taking anti-anemic drugs – the development of anemia in diaphragmatic hernia is associated with chronic blood loss from eroded mucosa;
- use of sorbents and prokinetics – in case of reflux of duodenal contents into the esophagus.
These principles apply to the most common variant of diaphragmatic hernia, the axial variant. Paraesophageal hernias, which account for about 1.5% of cases, are usually treated surgically. In elderly patients with severe pathologies that are contraindications for surgery, diet and lifestyle modification are important.
Surgical treatment
Indications for surgical treatment of diaphragmatic hernia are:
- the development of complications;
- The ineffectiveness of the conservative approach;
- paraesophageal type of hernia.
The main surgical options are:
- suturing of the hernia gate and additional fixation of the esophageal opening;
- suturing the stomach to the abdominal structures;
- Fundoplication – returning the final segment of the esophagus into the abdominal cavity, forming a cuff and suturing the hernia hole.
All these surgical procedures are performed in more than 550 hospitals around the world (https://doctor.global/results/diseases/diaphragmatic-hernia). For example, repair of a diaphragmatic hernia can be done in 26 clinic across Turkey for approximate price of $2.3 K (https://doctor.global/results/asia/turkey/all-cities/all-specializations/procedures/repair-of-diaphragmatic-hernia).
Prevention
Prevention may consist of the following:
- Pregravidar preparation to reduce the risk of congenital fetal malformations;
- Careful evaluation of patients after transportation accidents and other traumatic situations;
- Normalization of body weight and maintenance of weight within normal limits;
- timely treatment of constipation and chronic cough.
Rehabilitation
After the end of the main stage of treatment, patients are under the supervision of a gastroenterologist. Dynamic monitoring allows to prevent the development of complications, timely detection and treatment of reflux esophagitis.
